A busy ECMO hospital will often have three to five patients on ECMO at any given time. The number of patients using ECMO at Melbourne’s Alfred Hospital is roughly 20 virtually entirely due to COVID. In the US, hospitals report increased ECMO demand for teenagers and young adults with limited resources.
ECMO is a critical tool but it necessitates a large number of hospital resources and highly trained personnel. Patients who survive ECMO may develop long-term health problems as a result of their critical illness.
What Is ECMO? This Improved Life Support Is Shocking Doctors Now
The number of ICU patients on ECMO treatment has recently shocked doctors and health experts on social media. Extracorporeal membrane oxygenation (ECMO) is the last choice for individuals with severe cardiac and respiratory failure.
This is a critical situation for both the health care service providers and doctors as the patients need utmost care. In the peak covid situation, the demand for such treatment was very high and doctors across several states had a lot of troubles in providing the best treatment for patients.
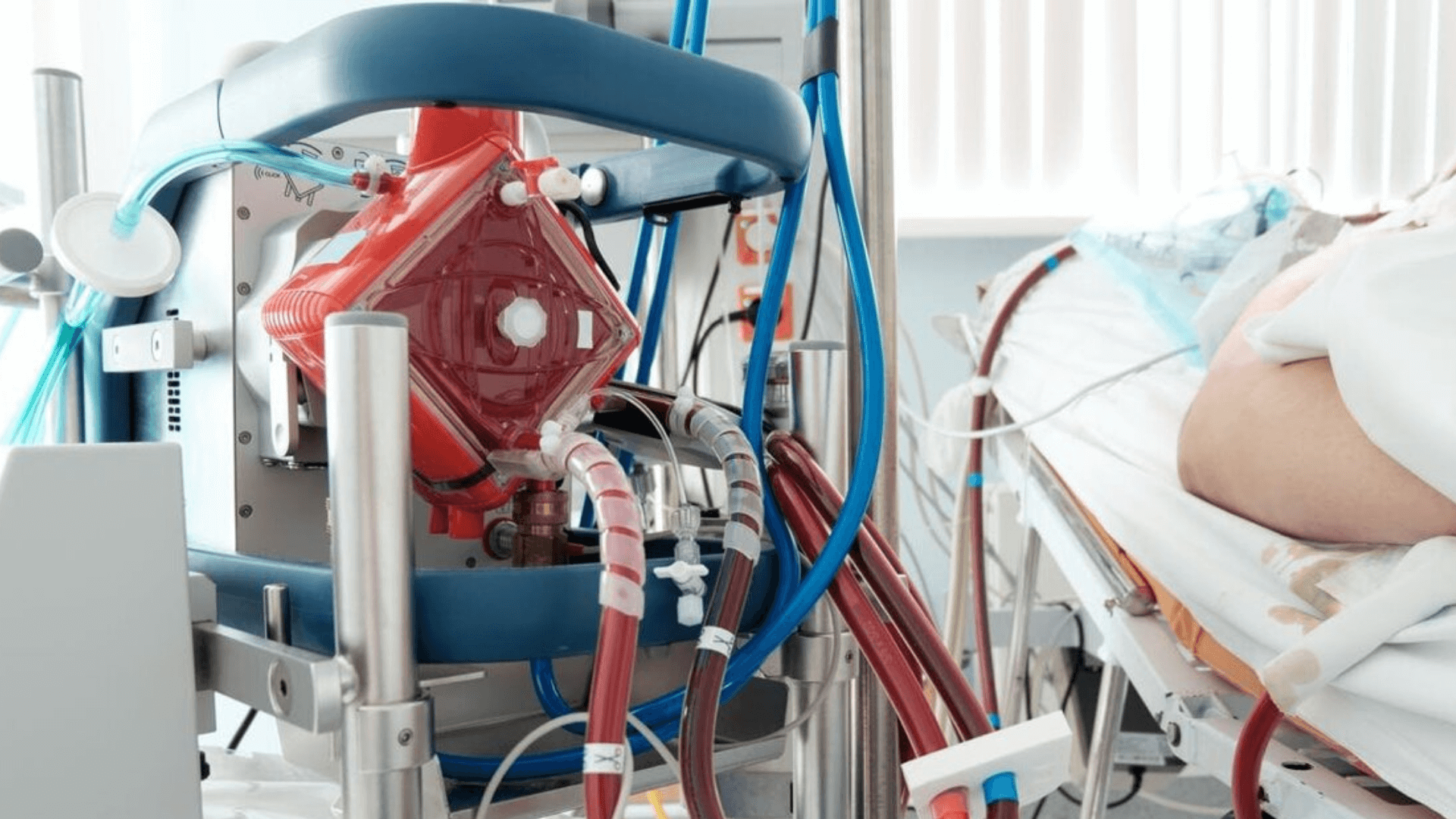
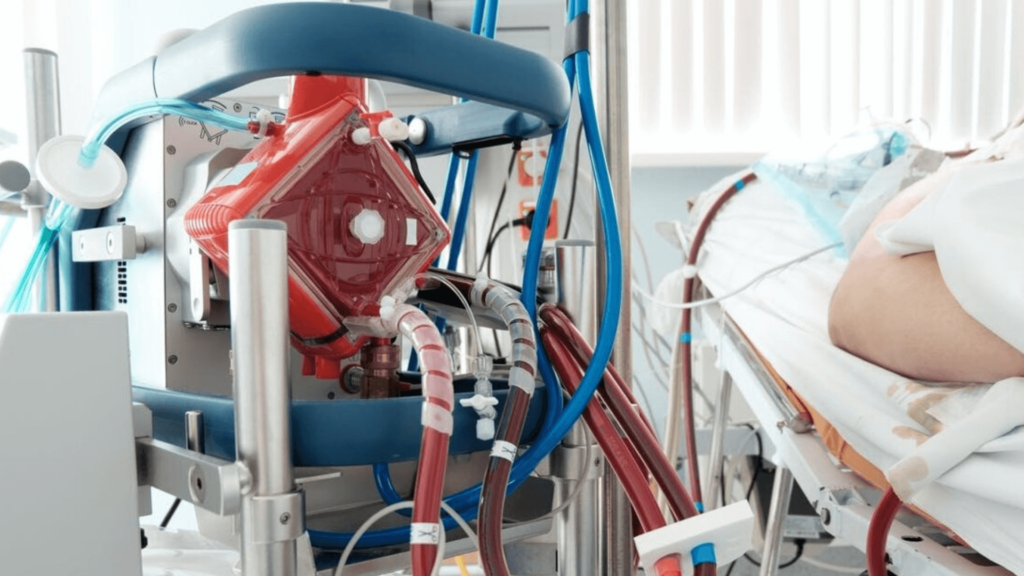
The heart and lungs are being outsourced.
ECMO stands for “extracorporeal membrane oxygenation” and refers to a heart or lung bypass machine. A pump and an artificial lung both located outside the body offer assistance that the ill organs are no longer capable of providing. All other bodily functions are kept intact.
Each letter in the ECMO acronym has the following meaning:
• Extracorporeal refers to something that exists outside of the body.
• Membrane: The artificial lung is made up of a “membrane” which is a thin layer of material that allows blood to flow on one side and oxygen to flow on the other. This porous thin membrane allows oxygen to pass through while allowing carbon dioxide to escape.
• Oxygenation: When oxygen is absorbed into the bloodstream it is the same as breathing in. The elimination of carbon dioxide which is similar to breathing out also occurs.
ECMO developed from cardiopulmonary bypass equipment used in open-heart surgery. However ECMO technology is designed to assist for days to weeks rather than hours.
ECMO can be connected to the patient in two ways: veno-venous and veno-arterial (to replace both the function of the patient’s lungs and the function of the patient’s lungs and the function of the patient’s lungs and the function of the patient’s lungs and the function of the patient.
Frequently this is only the beginning.
Even if a patient survives their first sickness they will most likely need continued hospital treatment and rehabilitation for several months later. To enhance the patient’s prospects of a good quality survival a full range of specialized hospital and rehabilitation therapies must be available.
Vaccination wearing a mask and keeping an eye on ventilation and air quality are all ways to keep yourself and our healthcare system safe from the spread of COVID illness.
Only a few facilities around the world including in Australia are capable of providing ECMO. All ECMO services in Australia are housed in large metropolitan critical care units (ICUs) while some ECMO retrieval services can start ECMO assistance in smaller hospitals before transferring patients to an ECMO ICU for continued care.
Highly skilled ECMO nurses give round-the-clock treatment. In many ECMO ICUs, one nurse is responsible for the ECMO machine while another is responsible for the patient who is still critically ill and is usually on a complete range of other life support measures in addition to ECMO. A ventilator to assist the lungs a dialysis machine to support the kidneys and a variety of medications supplied continually to keep the patient alive are examples of these.